The Brain and Spinal Cord
Tareq Yousef
The brain is a complex organ with billions of interconnected neurons and glia. These cells are the basis of communication in the nervous system, which is organised into specialised structures that provide the foundation for thought, emotion, and behaviour. In this section, we discuss the overall organisation of the nervous system and the functions associated with different areas, beginning with the spinal cord.
The Spinal Cord
The spinal cord connects the brain to the outside world. It works like a relay station to direct messages to and from the brain, and also has its own system of automatic processes, called reflexes.
The top of the spinal cord is a bundle of nerves that merges with the brain stem, where many basic life processes, like breathing and digestion, are controlled. The spinal cord itself ends just below the ribs while its nerves extend all the way to the base of the spine. It’s functionally organised into 31 segments, each connected to a specific part of the body through the peripheral nervous system. Nerves branch out from the spine at each vertebra: sensory nerves bring messages in; motor nerves send messages out to the muscles and organs.
The spinal cord is set up to make simple decisions about incoming sensory messages without requiring input from the brain. This is the basis of several types of reflexes, such as knee jerk and pain withdrawal reflexes. When a sensory message meets certain parameters, its signal passes from the sensory nerve to a spinal interneuron, which then activates a motor neuron to initiate movement. This happens before the brain receives information about the painful stimulus, so this automatic spinal reflex allows the body to react very quickly (and minimise injury!).
The spinal cord is protected by bony vertebrae and cushioned in cerebrospinal fluid, but injuries can still occur. When the spinal cord is damaged in a particular segment, all lower segments are cut off from the brain, usually causing paralysis and loss of sensation. Therefore, someone with a severe spinal injury at the level of the hips will keep motor control and sensation in more body parts than someone with a spinal injury at the level of the shoulders. The higher the damage occurs, the greater the loss of function and sensation. Below we will discuss the hindbrain, midbrain, and forebrain, as well as some important functional regions of the brain.
Hindbrain Structure
The hindbrain is located at the back of the head and looks like an extension of the spinal cord. It contains the medulla, pons, and cerebellum (Figure BB.9). The medulla controls the automatic processes of the autonomic nervous system, such as breathing, blood pressure, and heart rate. The word pons literally means “bridge,” and as the name suggests, the pons connects the hindbrain to the rest of the brain. Acting as a bridge, the pons contains several “highways” that send information about body sensations to the brain and brings directions for body movement down to the spinal cord. The pons is also involved in regulating sleep and pain signals. The medulla and pons are part of the brain stem, which extends to the thalamus in the forebrain.

Midbrain Structures
The midbrain, located between the forebrain and the hindbrain, is home to a curious collection of structures involved in diverse functions. The superior colliculus is important in directing eye movements towards important aspects of a visual scene, while the inferior colliculus is involved in sound localization. Both structures direct behaviours to parts of the environment that are relevant to an individual at that moment in time. The midbrain also contains structures that are involved in the sleep/wake cycle, arousal, and motor activity.
These structures include the substantia nigra (Latin for “black substance”) and the ventral tegmental area (VTA) (Figure BB.10), which both contain cell bodies that produce the neurotransmitter dopamine and project to areas of the forebrain.The substantia nigra is important for planning and control of voluntary movement, and degeneration of these dopaminergic (“-ergic” means that those neurons contain and can release the neurotransmitter, here, dopamine) neurons is thought to be the main cause of the neurological disorder, Parkinson’s disease (Parent & Parent, 2010). In terms of the VTA, it sends parallel projections to the forebrain and is involved in reward and motivation. Alterations in the neuronal signalling in this pathway is linked to addictive behaviours, such as substance misuse and gambling (George & Le Moal, 2012).

Forebrain Structures
The surface of the forebrain is dominated by the cerebral cortex, with its distinctive pattern of folds or bumps, known as gyri (singular: gyrus), and grooves, known as sulci (singular: sulcus), shown in Figure BB.11. These gyri and sulci allow us to separate the brain into functional centres. The most prominent sulcus, known as the longitudinal fissure, is the deep groove that separates the brain into two halves or hemispheres: the left and the right.

The cerebral cortex makes up the majority of the forebrain (Figure BB.12), the largest part of the brain. In addition to the cortex the forebrain contains a number of other subcortical structures including the thalamus, hypothalamus, pituitary gland, and a collection of areas called the limbic system. We will elaborate on these terms below, but first we will map out the lobes of the cerebral cortex.
, midbrain (a small central portion), and hindbrain (a portion in the lower back part of the brain).")
Watch this video: Tricky Topics: Cortical Anatomy (11 minutes)
“Tricky Topics: Cortical Anatomy” video by FirstYearPsych Dalhousie is licensed under the Standard YouTube Licence.
Here is the Tricky Topics: Cortical Anatomy transcript.
Lobes of the Cerebral Cortex
There are four lobes on each side of the cerebral cortex: frontal, parietal, temporal, and occipital (Figure BB.13). As its name suggests, the frontal lobe is located at the front and extends back to a fissure called the central sulcus, which separates it from the parietal lobe just behind. The temporal lobe begins below the lateral sulcus and extends backward towards the occipital lobe, which makes up most of the back part of the brain. The cortex can be described anatomically in terms of these lobes and sulci; size, shape, and location are all anatomical features that help us further map out different regions. Different areas of the cortex can also be described functionally, in terms of what they do. By the end of this section, you should be able to describe and compare different areas of the cortex both functionally and anatomically.

The size and location of the cerebral cortex makes it vulnerable to damage from injury and disease, however this is not usually fatal. In fact, most of what we’ve learned about the human cortex comes from observations of people living with damage to specific areas. If someone loses function after a brain injury, the damaged area was probably involved in that function.
Potentially the most famous case of brain damage is Phineas Gage: On September 13, 1848, 25-year old Gage was working as a railroad foreman. He and his crew were using an iron rod to tamp explosives into a blasting hole to remove rock along the railway’s path. Unfortunately, this created a spark and the rod exploded out of the hole, into Gage’s face, and through his skull (Figure BB.14). It passed through the left frontal lobe and exited between the parietal and frontal bones of the skull.
 is a photograph of Phineas Gage holding a metal rod. Image (b) is an illustration of a skull with a metal rod passing through it from the cheek area to the top of the skull.")
Remarkably, Gage was conscious and capable of moving and talking within minutes. In the following months he had a severe fungal infection of the brain (that could have resulted in more damage) and was cared for by doctor John Martyn Harlow (Harlow, 1848). Harlow’s notes provide the most direct information on Gage’s recovery.
In the months following the injury, Harlow wrote that Gage was improving, but he had trouble with self control. His friends also noted this with reports of overspending and inappropriate social behaviour, like swearing (Harlow, 1968). Within three months Gage was healthy enough to move home, but hadn’t recovered enough to resume his duties as a foreman. However, just four years later he moved to Chile to establish a line of stage coaches. The job involved scheduling, managing finances, and interacting with passengers during long journeys — requiring a lot of patience and perseverance! It seems unlikely that this would have been possible for the rude, unpredictable man often described in this case (Macmillan & Lena, 2010).
Harlow didn’t have access to imaging technology so we aren’t sure what structures were affected by Gage’s injury, or which structures adapted so he could recover. Luckily, we can use modern techniques to make an educated guess about what happened to Gage’s brain. A study from 2012 (Van Horn et al., 2012) used Gage’s skull along with imaging data from similar living subjects to model the damage based on the rod’s trajectory (Figure BB.15). This model suggested that the left orbitofrontal cortex in the frontal lobe was severely damaged. The majority of connective pathways from the left frontal lobe to other areas, including the limbic system, were also affected. Further inspection of Gage’s skull indicates that there may have also been some direct damage to the amygdala (Szczepanski & Knight, 2014).
 is a photograph of Phineas Gage holding a metal rod. Image (b) is an illustration of a skull with a metal rod passing through it from the cheek area to the top of the skull.")
So what kind of impairments do we commonly see after damage to these areas? Patients with damage to similar areas of the prefrontal cortex show higher scores on tests of impulsivity, taking less time to consider tasks and plan action, and making more errors. These patients are also less likely to change their behaviour in response to consequences, report more inappropriate social behaviours, and more feelings of anger (Berlin et al., 2004, Szepanski & Knight, 2015), similar to what Gage experienced. In fact, Harlow’s research with Gage prompted him to coin the term Frontal Lobe Syndrome, a term describing deficits in motivation, planning, social behaviour, and language production that can appear after damage to the prefrontal cortex (Pirau & Lui, 2021). Gage’s case provides a memorable demonstration of frontal lobe function, but it also shows the brain’s remarkable ability to adapt and regain function after injury.
This recovery illustrates neuroplasticity—the brain’s capacity to reorganize itself by forming new connections after damage or experience. When one region is injured, other areas can sometimes adapt to take over its functions, especially with practice and environmental support. Although plasticity is strongest in childhood, it continues throughout life, enabling people to recover skills, adapt behavior, and acquire new abilities (Kolb & Gibb, 2011). Gage’s partial recovery suggests that plasticity helped compensate for damaged frontal circuits, allowing him to regain social and occupational functioning. Beyond injury, plasticity underlies everyday learning: practicing a musical instrument rewires sensory and motor regions (Pascual-leone, 2001), learning a second language increases gray matter in memory and language areas (Mechelli et al., 2004), and even learning to juggle alters brain structure and connectivity (Draganski et al., 2004).
Brain damage studies provide important information about the cortex but advancements in medicine and technology have since given us more precise methods for investigating the brain. A foundational example comes from neurosurgeon Wilder Penfield, who systematically studied the effects of electrical stimulation on different parts of the cortex. At the very back end of the frontal lobe, just before the central sulcus, is a strip of cortex called the precentral gyrus and is home to the primary motor cortex, an area that activates movements after we decide to make them. Most of what we know about this part of the brain comes from classic research in epilepsy patients done by Penfield and associates Theodore Rassmussen and Edwin Boldrey.
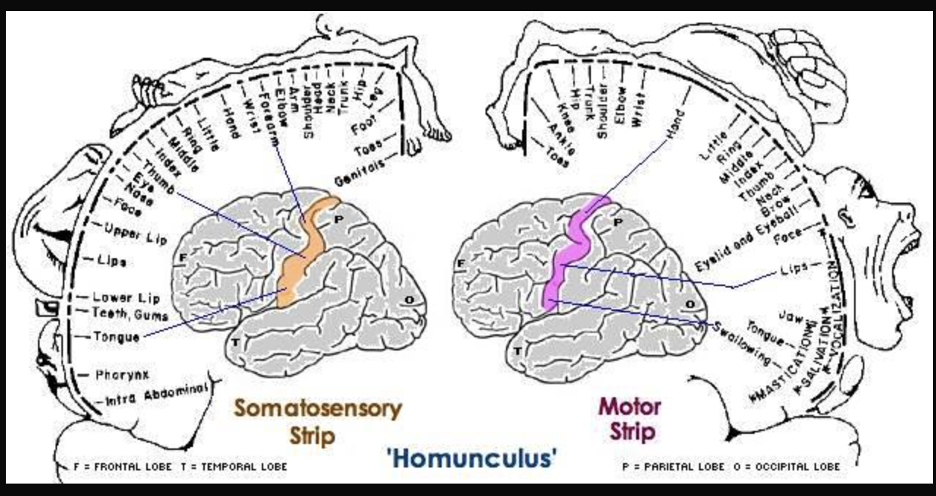

Just behind the motor cortex on the other side of the central sulcus is the primary somatosensory (involved in sensation of the body) cortex. This strip of cortex is at the beginning of the parietal lobe, and it plays an essential role in the perception of touch, temperature, and pain. Penfield discovered that electrical stimulation of this area produces tactile sensations in different regions of the body on the contralateral side. Like in the primary motor cortex, neurons in the primary somatosensory cortex are also grouped by body part, so that the arrangement in the body is maintained on the surface of the cortex (Figure BB.16).
Note that the size of body parts on both these motor and touch maps is distorted, with huge amounts of cortical space devoted to the fingers, hands, and mouth compared to the arms, legs, and torso (Penfield & Boldery, 1937; Penfield & Rasmussen, 1950). The areas of the body that we have more control over or which are more sensitive have the most cortical space. For example, the fingers have more cortical space than the chin, which is much less sensitive and can’t carry out coordinated movement.
Penfield’s representation of the brain’s somatosensory “touch map” as a two-dimensional homunculus or ‘little man’ is one of the most recognisable images in neuroscience. Every introductory Psychology textbook has some version of it, along with its twin, the “motor map”, located next door in the frontal lobe. These images demonstrate that 1) the map of the body is retained in the brain and 2) the size of a body part’s representation is related to its function rather than its physical size. These features are key to understanding the way movement and somatosensation are coded in the brain.
Other Areas of the Forebrain
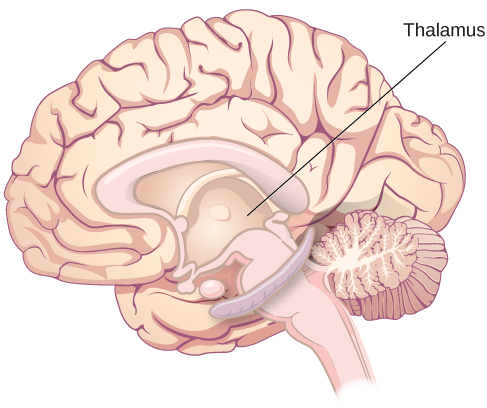
Other areas of the forebrain, located beneath the cerebral cortex, include the thalamus and the limbic system. The thalamus is a sensory relay for the brain. All of our senses, with the exception of smell, are routed through the thalamus before being directed to other areas of the brain for processing (Figure BB.18).
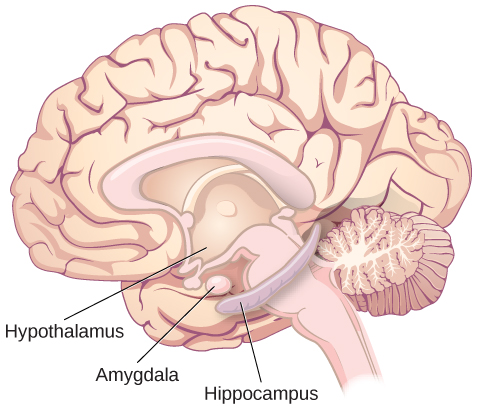
The limbic system is involved in processing both emotion and memory. The limbic system is made up of a number of different structures, but three of the most important are the hippocampus, the amygdala, and the hypothalamus (Figure BB.19). The hippocampus is an essential structure for learning and memory. The amygdala is involved in our experience of emotion and in tying emotional meaning to our memories. The hypothalamus regulates a number of homeostatic processes, including the regulation of body temperature, appetite, and blood pressure. The hypothalamus also serves as an interface between the nervous system and the endocrine system and in the regulation of sexual motivation and behaviour, all things that can also influence our emotion and learned behaviours (i.e., creation of new memories). You will read more about how learning happens shortly, and later on in this book!
Lateralization
You may be familiar with the idea that the right and left hemispheres have different abilities or specialised functions, referred to as lateralization. Some of the earliest evidence of lateralization comes from Paul Broca. Broca identified a structure in the frontal lobe now known as Broca’s area, which typically appears on the left hemisphere (Figure BB.21). This discovery came from work with patients with a particular set of language impairments after damage in the Broca’s area, called Broca’s aphasia.
Consider Louis Leborgne or ‘Tan’, Broca’s first patient with damage in this area. Leborgne was described as intelligent, and understood language but wasn’t able to reply with anything other than “tan” or a single swear word if he was angry. Leborgne’s primary communication was a combination of gestures and “tan”, spoken in a variety of tones depending on context (Devinsky & Samuels, 2016). This is why Broca’s aphasia is also called expressive aphasia, because people affected by it cannot produce communicative language in a verbal or written form, though they have no problems with comprehension.
Wernicke’s area, important for speech comprehension, is also located in the left hemisphere, close to the primary auditory cortex. Whereas individuals with damage to Broca’s area have difficulty producing language, those with damage to Wernicke’s area can produce words, but they aren’t able to understand language or combine words in sensible ways (Figure BB.21). In most people, both Broca’s area and Wernicke’s area are located in the left hemisphere.

These kinds of cases indicate that the left hemisphere may have some specialised control of verbal language. For most people, the left hemisphere is needed for verbal language, while the right hemisphere may be better at some kinds of comprehension and symbol recognition (Taylor & Regard, 2003). It’s likely that both hemispheres need to interact to produce a full range of language functions.
More evidence for lateralization comes from Michael Gazzaniga and his colleagues, who studied the function of each hemisphere independently in patients who had undergone ‘split-brain’ surgery. This surgery is used to stop the spread of seizures from one hemisphere to the other in some cases of severe epilepsy. To accomplish this the surgeon must cut the corpus callosum, a band of about 200 million axons that allows for communication between the two hemispheres (Figure BB.22). Because the two sides normally share the information they have processed, we aren’t aware of the different roles they play in day-to-day function.
This is not the case for split-brain patients. For instance, if you show a picture to the patient’s left visual field only, they won’t be able to name it because the information is only available in the largely nonverbal right hemisphere. However, they can recreate the picture with their left hand, which is also controlled by the right hemisphere. When the more verbal left hemisphere sees the picture that the hand drew, the patient is able to name it (assuming the left hemisphere can interpret what was drawn by the left hand).
 and (b) show the corpus callosum’s location in the brain in front and side views. Photograph (c) shows the corpus callosum in a dissected brain.")
More data from Gazzinga and associates suggests that a variety of functions show patterns indicating some degree of hemispheric dominance (Gazzaniga, 2005). For example, the left hemisphere may be superior for forming associations in memory, selective attention, and positive emotions. The right hemisphere, on the other hand, may be superior in pitch perception, arousal, and negative emotions (Ehret, 2006). It’s tempting to conclude that certain behaviours can be attributed to one hemisphere or the other, but research in this area produces inconsistent results and there’s a natural variation of brain organisation in every population of humans (Banich & Heller, 1998).
Watch this video: Tricky Topic: Hemispheric Lateralization (9 minutes)
“Tricky Topics: Hemispheric Lateralization” video by FirstYearPsych Dalhousie is licensed under the Standard YouTube licence.
Here is the Tricky Topics: Hemispheric Lateralization transcript.
By the end of this chapter, you are encouraged to take time to reflect on the physical parts of you that make you who you are. The sum of all of the parts of your nervous system (from the neurotransmitters to the synapses they target, the axons of neurons that carry electrical signals, and beyond) make up a vastly complex organism that not only responds to its environment, but has thoughts and feelings. How vast and brilliant! Many psychologists aim to understand how this all works, an opportunity you will have if you continue on in this field.
Summary
Cells of the Nervous System
Glia and neurons are the two cell types that make up the nervous system. While glia generally play supporting roles, the communication between neurons is fundamental to all of the functions associated with the nervous system. Neuronal communication is made possible by the neuron’s specialised structures. The soma contains the cell nucleus, and the dendrites extend from the soma in tree-like branches. The axon is another major extension of the cell body; axons are often covered by a myelin sheath, which increases the speed of transmission of neural impulses. At the end of the axon are terminal buttons that contain synaptic vesicles filled with neurotransmitters.
Neuronal communication is an electrochemical event. The dendrites contain receptors for neurotransmitters released by nearby neurons. If the signals received from other neurons are sufficiently strong, an action potential will travel down the length of the axon to the terminal buttons, resulting in the release of neurotransmitters into the synaptic cleft. Action potentials operate on the all-or-none principle and involve the movement of sodium (Na+) and potassium (K+) across the neuronal membrane.
Different neurotransmitters are associated with different functions. Often, psychological disorders involve imbalances in a given neurotransmitter system. Therefore, psychotropic drugs are prescribed in an attempt to bring the neurotransmitters back into balance. Drugs can act either as agonists or as antagonists for a given neurotransmitter system.
Parts of the Nervous System
The brain and spinal cord make up the central nervous system. The peripheral nervous system comprises the somatic and autonomic nervous systems. The somatic nervous system transmits sensory and motor signals to and from the central nervous system. The autonomic nervous system controls the function of our organs and glands, and can be divided into the sympathetic and parasympathetic divisions. Sympathetic activation prepares us for fight or flight, while parasympathetic activation is associated with normal functioning under relaxed conditions.
The Brain and Spinal Cord
The brain consists of two hemispheres, each controlling the opposite side of the body. Each hemisphere can be subdivided into different lobes: frontal, parietal, temporal, and occipital. In addition to the lobes of the cerebral cortex, the forebrain includes the thalamus (sensory relay) and limbic system (emotion and memory circuit). The midbrain contains the substantia nigra and ventral tegmental area. These structures are important for movement, reward, and addictive processes. The hindbrain contains the structures of the brainstem (medulla, pons, and midbrain), which control automatic functions like breathing and blood pressure. The hindbrain also contains the cerebellum, which helps coordinate movement and certain types of memories.
Individuals with brain damage have been studied extensively to provide information about the role of different areas of the brain, and recent advances in technology allow us to obtain similar information by imaging brain structure and function. These techniques include CT, PET, MRI, fMRI, and EEG.
Cerebellum:
(i.e., little brain) Consists of two wrinkled ovals behind the brain stem. It functions to coordinate voluntary movement.
Medulla:
The area of the brain stem that controls heart rate and breathing.
Pons:
A structure in the brain stem that helps control the movements of the body, playing a particularly important role in balance and walking.
Cerebral Cortex:
The outer bark-like layer of our brain that allows us to so successfully use language, acquire complex skills, create tools, and live in social groups. The aspect of the brain that sets humans apart from other animals.
Pituitary Gland:
A pea-sized gland located near the centre of the brain that also known as the “master gland”. The pituitary gland is responsible for controlling the body’s growth, as well as secreting hormones that signal the ovaries and testes to make sex hormones and influence our responses to pain. The gland also controls ovulation and the menstrual cycle in women and is important in regulating behaviour.
Limbic System:
A brain area, located between the brain stem and the two cerebral hemispheres, that governs emotion and memory. The system includes the amygdala, the hypothalamus, and the hippocampus.
Frontal Lobe:
A portion of the brain located behind the forehead, also known as the motor cortex, that is involved in motor skills, higher level cognition (thinking, planning, memory, and judgment), and expressive language.
Parietal Lobe:
A portion of the brain that extends from the middle to the back of the skull, also known as the somatosensory cortex, that is involved in the processing of other tactile sensory information (information about touch).
Temporal Lobe:
A portion of the brain, also known as the auditory cortex, Located in front of the occipital lobe between the ears. It is involved in the interpretation of the sounds and language we hear.
Occipital Lobe:
A portion of the brain, also known as the visual cortex, that is involved in interpreting visual stimuli and information.
Motor Cortex:
The part of the cortex that controls and executes movements of the body by sending signals to the cerebellum and the spinal cord.
Somatosensory Cortex:
An area just behind and parallel to the motor cortex at the back of the frontal lobe, receives information from the skin’s sensory receptors and the movements of different body parts.
Thalamus:
An egg-shaped structure above the brain stem that applies more filtering to the sensory information that is coming up from the spinal cord and through the reticular formation, and relays some of these remaining signals to the higher brain levels.
Hippocampus:
Located within the limbic system and consists of two “horns” that curve back from the amygdala. Important for the storage of information in long-term memory.
Amygdala:
Located within the limbic system. This structure consists of two “almond-shaped” clusters and is primarily responsible for regulating our perceptions of, and reactions to, aggression and fear.
Hypothalamus:
A brain region that is located in the lower, central part of the brain that is responsible for synthesizing and secreting hormones and plays an important role in eating behavior.
Brain Lateralization:
The idea that the left and the right hemispheres of the brain are specialized to perform different functions.
Broca’s Area:
An area in front of the left hemisphere near the motor cortex responsible for language production.
Wernicke’s Area:
An area of the brain next to the auditory cortex responsible for language comprehension.
Corpus Callosum:
The region that normally connects the two halves of the brain and supports communication between the hemispheres.
